Hospital Clínic de Barcelona, Spain
Hospital Clínic de Barcelona has been a leading public healthcare provider in the city of Barcelona, (Catalonia, Spain) for over 100 years. It is a university hospital, developed together with the Faculty of Medicine of the University of Barcelona.
Healthcare, research, and teaching are their three main areas of actions which, together with the deep commitment to excellence that characterizes all the people who work there, make Hospital Clínic a well-known center of excellence not only in the country but also all over the world.
The Cardiovascular Institute of Hospital Clínic de Barcelona (ICCV) is the healthcare area dedicated to treating cardiovascular diseases.
All professionals who work at Cardiovascular Institute offer top quality healthcare assistance to people that come to their institute. As the entire hospital, it is located in the town center of Barcelona, representing a perfect combination between tradition and innovation. Localized in the beating heart of the city, the hospital was built close to the historical building of the University Faculty of Medicine. Here, ICCV professionals teach several subjects in bachelor’s degree courses in Medicine, Nursing and Biomedical Engineering. The institute therefore has a story that starts more than one century ago, representing a great example of tradition of a European university hospital. From that day, clinical activities have been carried out with an increasing attention to cardiovascular research and technological innovation, that now makes ICCV one of the most advanced and state-of-the-art hospitals in the world.
From 2021, the Cardiovascular Institute of Hospital Clínic began to renew its operatory area. All the spaces were completely redesigned to modernize all technologies, including the two existing angiography suites. In addition to them, a new hybrid room has been designed, intended to support mostly an ever-growing number of structural heart procedures. The two angiography rooms were completely transformed and equipped by two Innova IGS520 with Autoright, the AI-based image chain that automatically works in real time to optimize IQ & dose. For the hybrid room, ICCV has chosen the latest system of the GE Family, Allia IGS7 with Autoright, becoming the first European site installing this innovative robotic system in a cardiovascular hybrid room.

From 2015, Prof. Marta Sitges is the director of the Cardiovascular Institute at Hospital Clínic. We asked her to introduce us to their Institute and to tell us about the activities they routinely carry on there.
Prof. Marta Sitges : Our institute is dedicated to cardiovascular patient care based on three specialties: vascular surgery, cardiovascular surgery and cardiology. There are more than 60 medical professionals working here, along with more than 300 nursing and administrative support professionals. Every year we handle 3000 interventions, in addition to countless cardiovascular consultations.
We can count on a wide variety of multi-modalty imaging capabilities that allow us to carry out a wide range of cardiovascular diagnoses and interventions, which goes from percutaneous to surgical treatments.
Why did you make the decision to incorporate a hybrid room?
Prof. Marta Sitges : In recent years, cardiovascular medicine has evolved in such a way that the same disease can be treated with different approaches: in a minimally invasive manner, percutaneously, with open surgery, with medical treatments and so on. The need to work with multidisciplinary teams is evident in the field of cardiovascular diseases, especially for example on heart valve interventions or on some arrhythmias’ treatments. In these cases, to offer the patient the best care, we combine different techniques with different accesses. For this, it is essential to have a hybrid interventional room in which open surgery procedures can be simultaneously combined with percutaneous interventional procedures, keeping always in mind patient’s safety.
Why did you choose Allia system for your new hybrid operating theatre?
Prof. Marta Sitges : We have been working with General Electric for many years in the field of echocardiography, cardiac resonance, and electrocardiographic monitoring. We have always noticed and felt that this is a company that takes care of its customers and provides support after a system has been purchased. In addition to that, with Allia General Electric offered us an extremely high-tech system, with technical characteristics that more than met our requirements.
What type of procedures are currently carried out in the hybrid room and what procedures are intended to be incorporated in the future?
Prof. Marta Sitges : At the moment we are using the hybrid operating theatre to carry out structural interventional procedures, transcatheter valve implantation procedures, percutaneous repairs to heart valves, atrial appendage closures and septal defects closures.
We are also aiming to incorporate vascular surgery procedures, which also require a hybrid approach combining open surgery with endovascular techniques.
In the future, we think we will be able to use this hybrid operating theatre to carry out procedures that are currently being developed, such as endocardial and epicardial hybrid ablation for atrial fibrillation. Maybe even some kinds of ventricular tachycardia could also be optimal interventions that we could perform in our center with our new Allia hybrid room.
In the Cardiovascular Institute at hospital Clínic also work Dr. Manel Sabaté and Dr. Xavier Freixa. Dr. Sabaté is head of the hemodynamics and interventional cardiology department, and he is mostly dedicated to the treatment of coronary heart disease and the most frequent valve diseases at aortic and mitral level. Dr. Freixa is an interventional cardiologist specialized in structural and adult congenital heart disease.
What do you value the most in a angiography system for your procedures?
Dr. Manel Sabaté : I think there are several points to keep in mind when treating patients, especially in the cardiac district. The first one is certainly radiological protection, both for the personnel treating the patient and the patient itself. Then, for sure a system needs to provide a proper and optimized image quality, which could be adapted to any procedural step.
How has your daily practice improved since you got the Allia system?
Dr. Xavier Freixa : I really think Allia has been a significant improvement for our Institute for three reasons. The first is that Allia provides great images, so we improved in image quality enormously compared to what we were used to. Thanks to Autoright feature, the system can adjust both the dose and IQ for you, and adapts to whatever you need in different procedural steps. The second is that being able to move the system around means we can configure the room considering the various equipment needed. Since Allia is not fixed either to the ceiling or to the floor, we are always able to find the perfect positioning so that we - as well as echo cardiologists, surgeons and anesthetists- have all got exactly the right amount of room to work in. This feature is always important, but it is key when you speak about structural procedures. Finally, Allia allows you to incorporate advanced software, and let you control it from right inside the theatre.
Speaking of image quality and dosimetry, which Allia innovations do you use to optimize this image quality/dose ratio?
Dr. Manel Sabaté : The Allia system really does have the ability to combine the two key things that I think are the most important during a procedure, which is maintaining good image quality and protecting both the patient and the staff from radiation.
During the procedure, with Allia you always know the dose you are giving the patient thanks to dose quantity speedometer systems. This feature has also the possibility to activate a dose limiter, that really helps us to control the dose you give the patient in real time. This way you can even customize the image quality you produce at different angulations during the procedure.
Finally, with Innovasense the detector adapts to the patient’s contour in safety conditions, which means that the amount of received and scattered radiation is much less.
Allia presents the possibility to move both the table and the C-arm from the buttons of the detector. What do you think about this new feature?
Dr. Xavier Freixa : It is great having the possibility to control all system movements, including table motions, even from the detector side. Being able to move things around in various areas means that different team members can work and move around the table without the need to go to each part of the theatre. This has given much more autonomy to us during the procedure.
Speaking about the Advanced Application portfolio, what benefits you find fundamental using image fusion?
Dr. Xavier Freixa : The truth is that the benefits of fusion imaging are obvious, in particular in all kinds of procedures where the morphology of the structures is important such as Transcatheter Aortic Valve Implantation, paravalvular leak closures, left atrial appendage closures and so on. Actually, fusion imaging with ASSIST packages is a huge help both with pre-op preparation and during the procedure. This way we are able to reduce the dose of contrast and radiation significatively.
In coronary procedures, more and more different imaging systems such as OCT, IVUS, etc. are regularly used. What do you think about the integration of these systems with Allia?
Dr. Manel Sabaté : Nowadays, when we are treating a coronary patient we need to be able to combine various imaging and coronary physiology systems. For instance, we can use Allia to capture the image we get at the same time using techniques such as OCT. We can even use Online QCA, and very easily carry out a really high-quality coronary quantitative analysis directly from the touch panel of the system. Coronary physiology images are very well integrated within the system.
The statements by GE HealthCare customers described here are based on their own opinions and on results that were achieved in the customer’s unique setting. Since there is no “typical” hospital and many variables exist, i.e. hospital size, case mix, etc., there can be no guarantee that other customers will achieve the same results.
Para-valvular leak closure in aortic mechanical valve
Courtesy of Dr. Freixa, Hospital Clínic de Barcelona
Patient History
70 years old female. Cardiovascular Risk Factors: Hypertension and Hyperlipidemia. Mitral and aortic mechanical valve replacement in 1995 (27 Carbomedics Mitral and 21 Carbomedics Aortic). LVEF 30%. Severe aortic paravalvular leak (PVL) at the left coronary sinus. Symptoms: Poor functional class (NYHA 3) with severe hemolytic anemia requiring blood transfusions every 1-2 weeks.
PVL Diagnosis
Transthoracic echo (TTE) and Angio-CT showing a 7x3 mm aortic PVL at the left coronary cusp
Preparation
Theatre Setup
The patient was placed headfirst with Allia at 0 degrees. Another option would have been to place it at 90 degrees, as either way allows easy access to the patient’s head for anesthetist and echocardiographer.

PVL Intervention
Procedure done with general anesthesia and guided by TEE and CT-Fluoro Fusion.
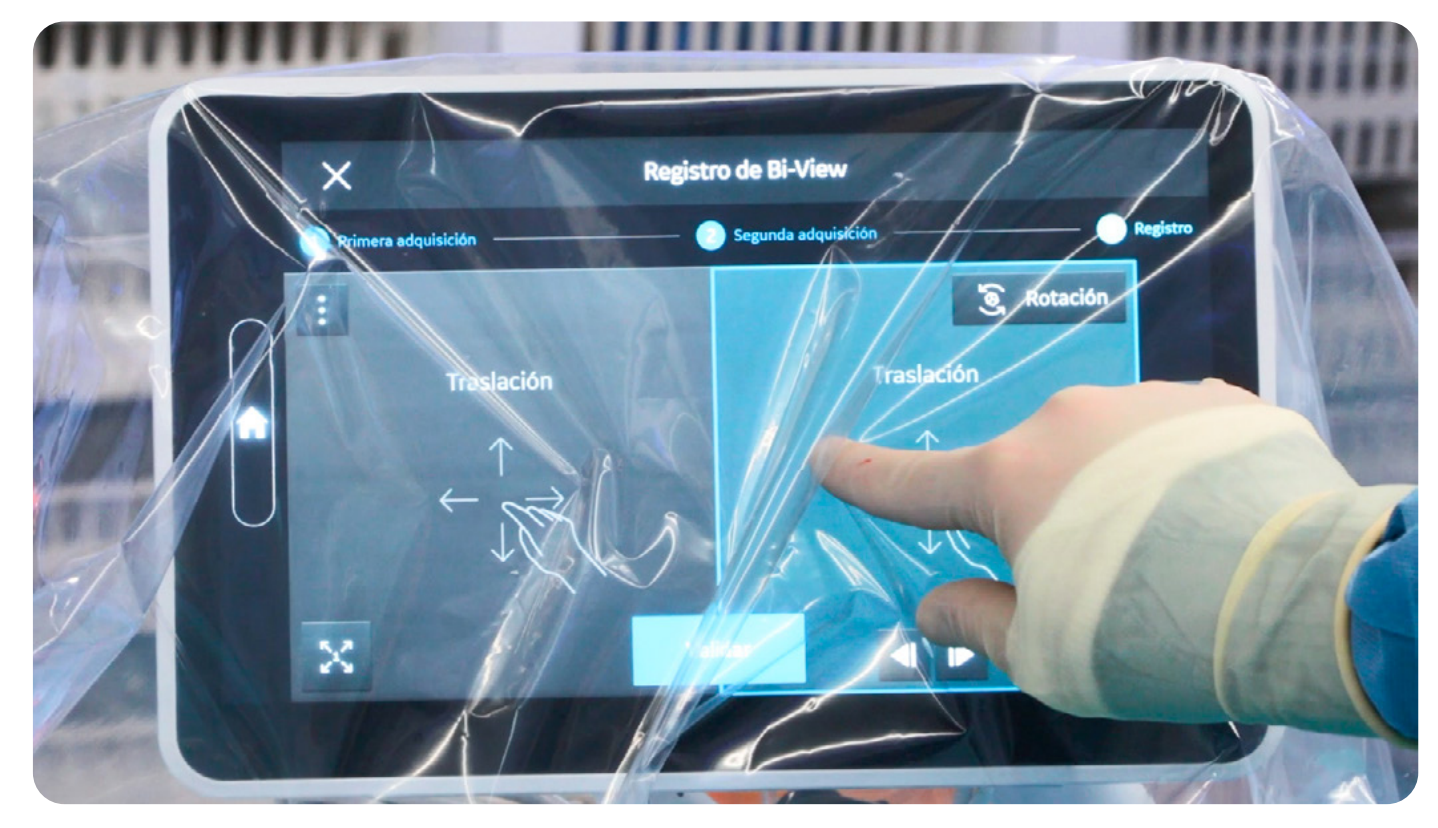
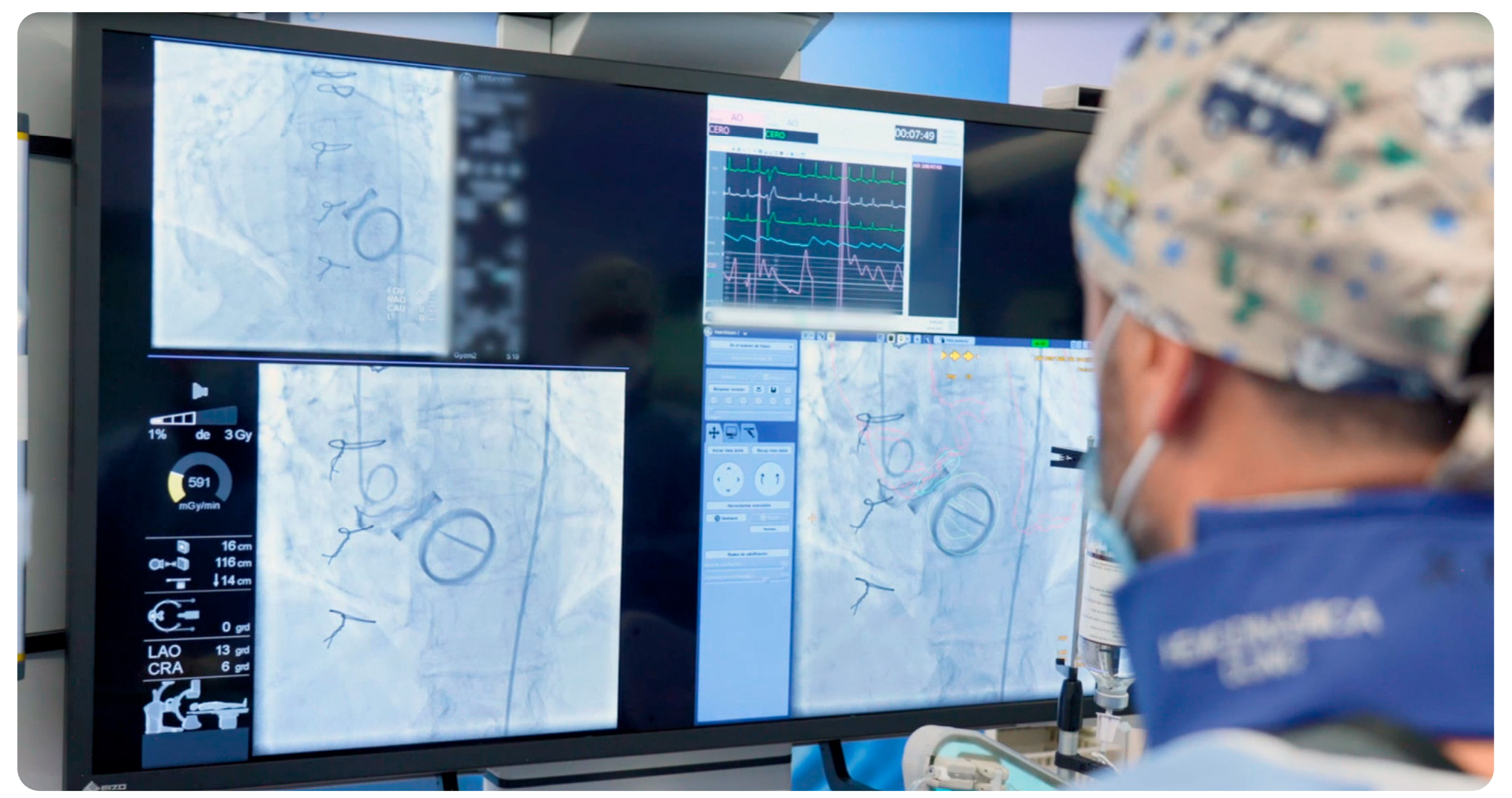
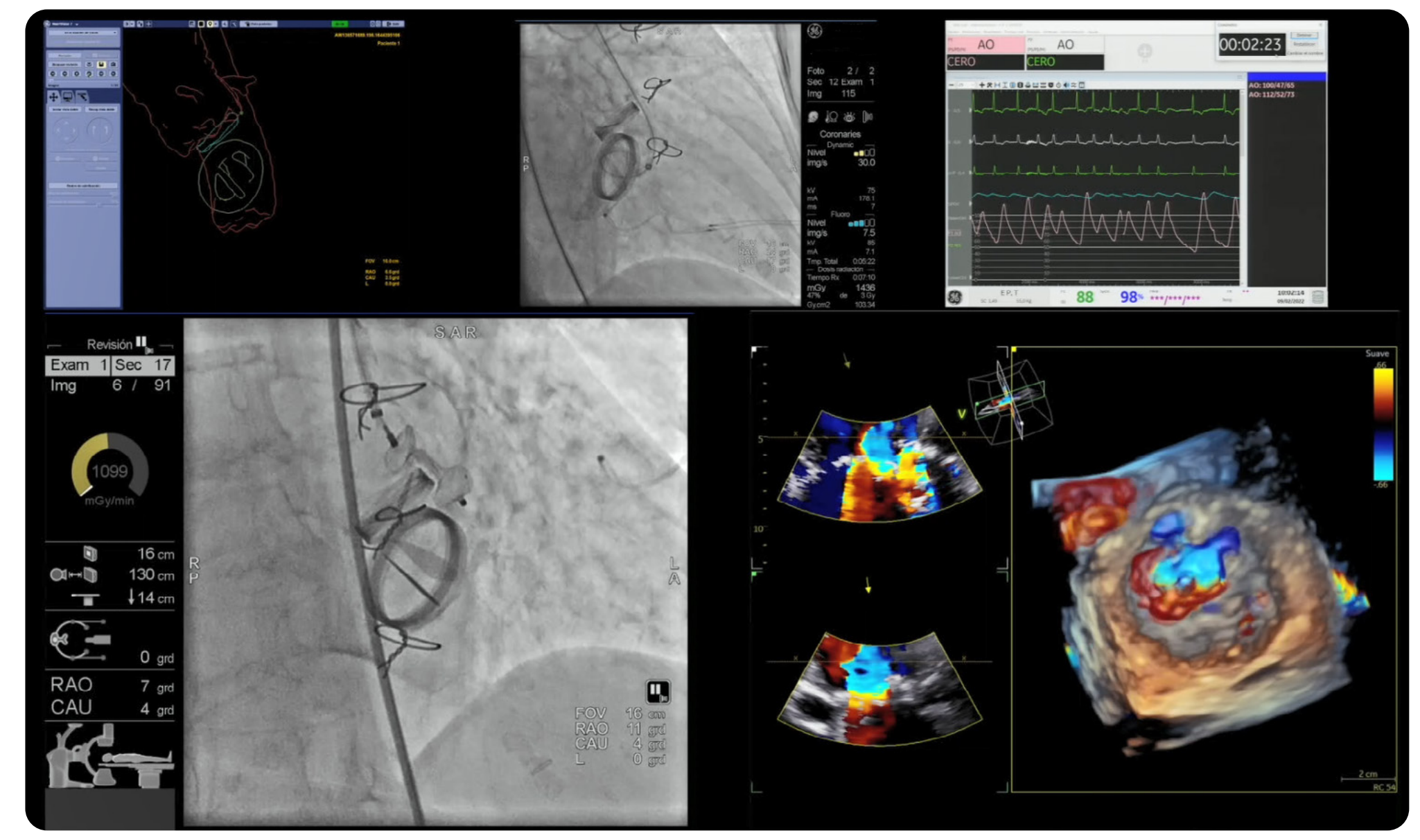
Acquisition parameters: Dynamic @15fps Level 2; Fluoro @7.5fps Level 3 with Dose Limiter on. A Large Display Monitor configuration with a big AW screen was used at the beginning of the procedure to perform the bi-view registration, which was easily performed at tableside with the touch panel using LAO/RAO fluoro images and the mechanical valves as anatomical landmarks.
Afterwards, the LDM layout was changed to show the U/S guidance.
“CT-Fluoro fusion was crucial to minimize radiation and contrast dose.”
Dr. Freixa
Access through the right femoral artery (6Fr). AL-1 (5Fr) and hydrophilic wire to cross the PVL and wire exchange with a high supportive Safari. Then, an AVP-3 14x5 mm through a 6Fr 110cm Flexor Catheter was successfully implanted at 24 RAO 17 CAU angulation.
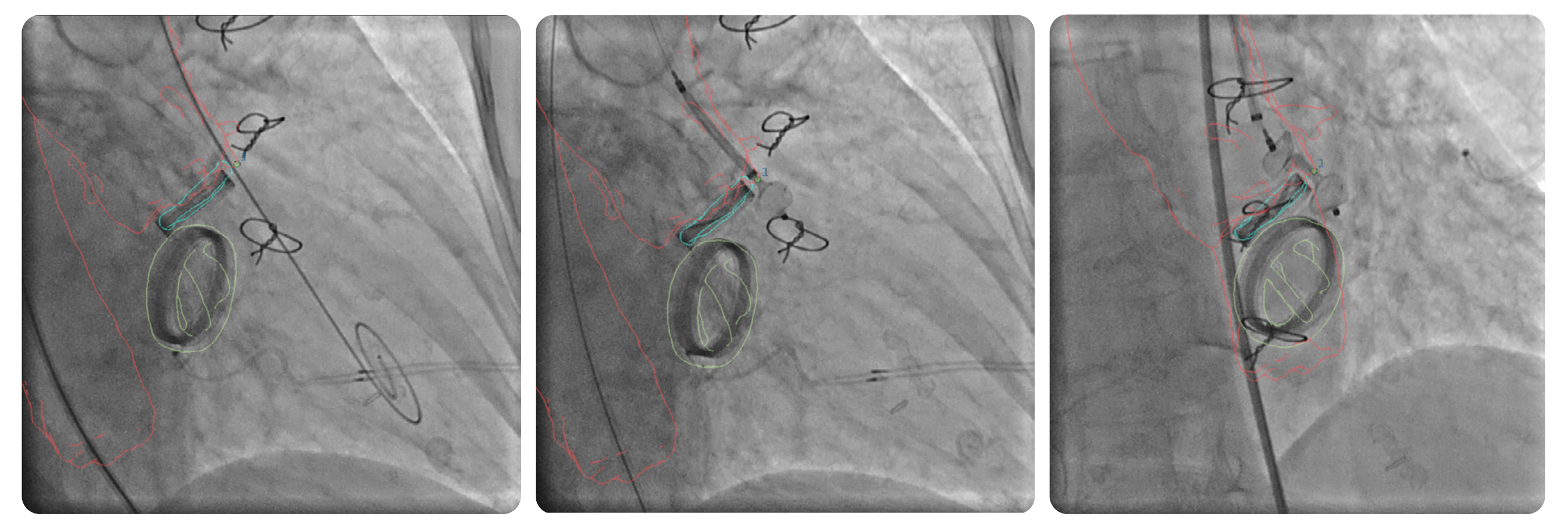
Good result with minimal residual leak. No interference with the mechanical valve or the left coronary artery.
Clinical Evolution
Clinical follow-up in 1 month showing a relevant clinical improvement with no more transfusions and good functional class (NYHA 1-2)
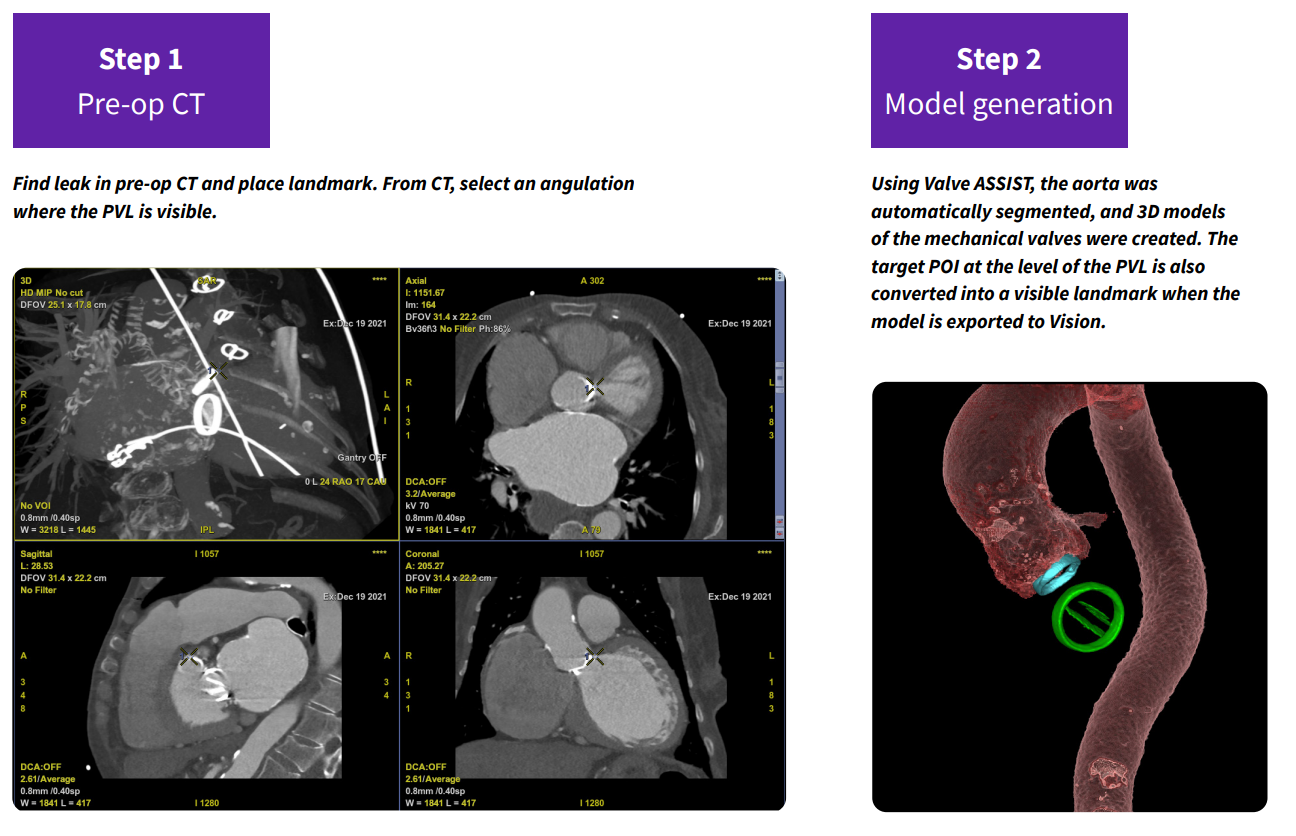
“The positioning of a marker at the level of the PVL allowed a very easy and straight forward leak crossing and identification of the best projection, that provided a better visualization of the plug implantation.” Dr. Freixa
The statements by GE HealthCare customers described here are based on their own opinions and on results that were achieved in the customer’s unique setting. Since there is no “typical” hospital and many variables exist, i.e. hospital size, case mix, etc., there can be no guarantee that other customers will achieve the same results. JB19335XX