
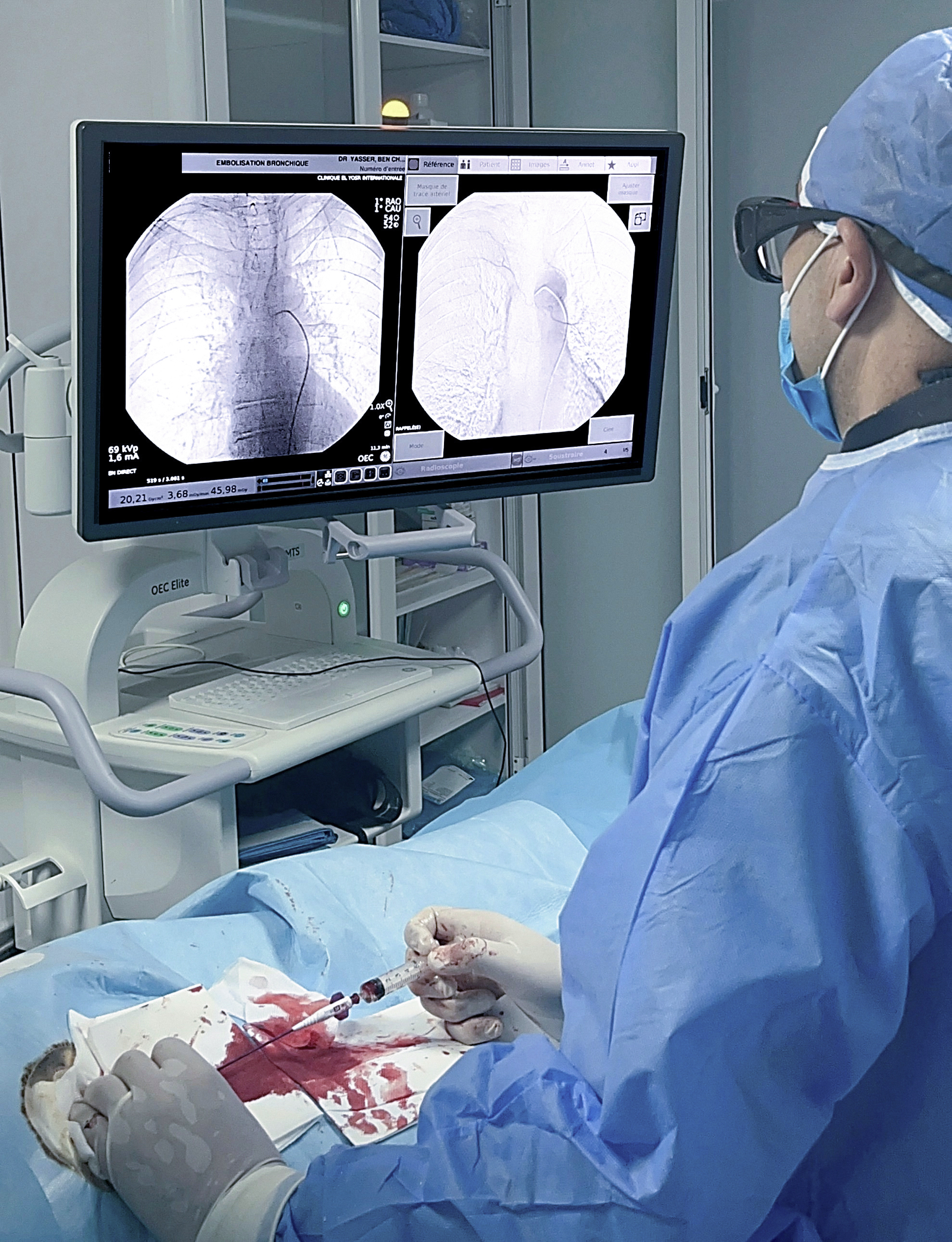
Interview with Dr. Yasser Ben Cheikh, Head of Interventional Radiology, Clinique El Yosr International, Sousse, Tunisia.
Located south of Tunis, overlooking the Gulf of Hammamet in the Mediterranean Sea, the city of Sousse is the third largest municipality in Tunisia. In the heart of this city with neo-Moorish architectural style, the El Yosr International clinic was founded in 2001. Offering a wide range of healthcare services, the clinic is expanding thanks to the dedication of its practitioners, developing new specialties, particularly in interventional radiology.
Thus, after a long career at the Sahloul University Hospital in Sousse, Dr. Yasser Ben Cheikh joined the El Yosr International Clinic to develop the interventional radiology unit’s care offerings. In search of an advanced mobile catheterization laboratory (cath lab) solution, Dr. Ben Cheikh opted for the OEC Elite CFD C-arm with motorized drive and remote control to equip his new cath lab room.
Dr. Yasser Ben Cheikh, MD and secretary of TIRA, the Tunisian Interventional Radiology Association, explains how OEC Elite CFD contributes to his daily work for Interventional Radiology procedures.
Dr. Ben Cheikh, what Interventional procedures do you perform in your mobile cath lab?
“The El Yosr International Clinic has a catheterization room equipped with a fixed imaging system, or fixed cath lab. As in many healthcare centers, its access is primarily reserved for interventional cardiologists who perform diagnostics and treatments for emergency procedures. So, when I joined the clinic, I wanted to have a catheterization room accessible at any time for my activities, right next to my consultation office.
This is why I opted for a mobile cath lab: a room equipped with a stateof-the-art mobile C-arm, allowing me to work peacefully without concerns regarding room availability. During my university career, I only worked in fixed cath labs. So, I had to adapt to my new mobile room and get used to the imaging output of the OEC Elite CFD C-arm. I started with simple procedures such as percutaneous access, biliary drainages, nephrostomies, and JJ stent placements. Then, I gradually increased the complexity of the procedures I performed in the mobile cath lab with peripheral endovascular acts and interventional procedures in the liver, such as chemoembolization, biliary drainages, and stent placements.
This progressive learning process has allowed me to perform procedures on the OEC Elite CFD mobile C-arm and today, I comfortably handle more complex procedures such as embolization of the portal system, hepatic venography, and embolization in various organs. For example, I quickly identify the Adamkiewicz artery and its different branches that nourish the spinal cord during bronchial embolization procedures. I can triage emergencies either in the mobile or the fixed cath labs without concerns, depending on the complexity of the procedure. It is a very good solution for hospitals that cannot afford to buy two fixed cath labs.”
What are the advantages of OEC Elite CFD C-arm for your mobile cath lab?
“For endovascular procedures in lower limbs, particularly below the knee (BTK) procedures, the image quality of OEC Elite CFD is excellent. The mobile cath lab is very good; allowing procedures to be performed quickly and with flexibility in the setup of the equipment in the operating room.
The motorization of OEC Elite CFD, controlled by myself with the remote user interface (RUI), provides great comfort during the procedure.
“The 31 x 31 cm flat panel detector, the large 4K UHD display, and the motorization of the C-arm that can be controlled remotely from the sterile field, make OEC Elite CFD closer to the performance of a small catheterization room than that of a traditional operating room C-arm.”
Dr. Yasser Ben Cheikh
With my RUl on the table’s rail and the workstation’s touch-screen, I am completely independent and can perform my entire procedure without needing to ask for help from the staff.
For more complex procedures, since I am familiar with my mobile equipment set up, I can adequately prepare my intervention plan. For example, for liver procedures, it is critical to know well the arterial and venous anatomy. Therefore, I study the patient’s preoperative CT scan more carefully than if I was working in a fixed room and I memorize the patient’s portal and arterial anatomy.
During the procedure, thanks to the use of the Live Zoom, I can navigate my catheter on the zoomed image of the anatomy while also viewing the entire non-zoomed anatomy on the second screen without increasing the dose to the patient. I can also automatically reposition the C-arm by recalling the preset oblique angles or position the C-arm in the desired viewing angle using the joystick of my RUI attached on the table’s rail.

In procedures where I need to embolize aneurysms or tumors, I use the different imaging protocols of OEC Elite CFD to search and to identify anastomoses. These protocols allow me to repeat selective injections of contrast agent at different concentrations to identify the target that I need to navigate my tools towards and treat. Thanks to the RUI, I can easily switch to low-dose or pulsed fluoroscopy mode or choose between the General HD or Vascular imaging profile. Indeed, the General HD profile enhances the contours of the guidewires and allows for more precise navigation during ultra-selective catheterization steps, for example.
In the future, I would like to offer to my patients hemorrhoid vein embolization procedures. This is a technique that is currently being validated, which appeared 10 years ago and is increasingly recommended by scientific societies. I observe a significant increase in the number of patients treated with this technique. The procedure is performed in the anatomy of the pelvis, which is a complex anatomy in radiographic imaging due to its density and its volume. It requires different viewing angles and different fluoroscopy modes. I am confident that I can do these embolization procedures in my mobile cath lab.

For other procedures such as chemoembolization of prostate arteries, it is necessary to perform a final control on volumetric images of the arteries via the acquisition of an injected CBCT. This is done to verify the result of the procedure due to variations in patient’s anatomies. Therefore, I perform these procedures in the fixed room. However, for many other procedures, the mobile cath lab with OEC Elite CFD in motorized configuration is more than sufficient.
“With OEC Elite CFD, I have all the imaging tools to perform hemorrhoid vein, portal system and other types of embolization procedures.”
Dr. Yasser Ben Cheikh
In summary, the image quality of OEC Elite CFD is truly very satisfying. My mobile cath lab is cost-effective because in Tunisia, the procedure’s billing is the same regardless of the type of room in which it is performed.”
“With my mobile cath lab equipped with OEC Elite CFD, I can carry out my activity independently and without worries.”
Dr. Yasser Ben Cheikh
 |
Dr. Yasser Ben Cheikh began his specialization in radiology in 2011 and quickly went into Interventional Radiology, completing various internships in Tunisia and in Nîmes, France. Upon returning to Tunisia in 2015, he joined the Sahloul University Hospital in Sousse in the Interventional Radiology department. After his internship, he took on the role of university hospital assistant and then Head of the Interventional Radiology Unit. By performing and training many colleagues in endovascular techniques, hepatic embolizations, percutaneous interventions, and arteriography, he helped develop a reimbursement system for interventional radiology procedures in Tunisia. In 2021, Dr. Ben Cheikh became head of the Interventional Radiology Unit at the El Yosr International Clinic in Sousse. He is the Secretary General of TIRA, the Tunisian Interventional Radiology Association. |
Complete portal embolization before right hepatectomy
Portal embolization is an interventional radiology procedure performed under general anesthesia. It is a specific embolization of the smallest capillaries of the portal system. It aims to deprive segments of the liver from their blood supply. This procedure is performed before hepatectomy, surgical resection of the liver’s segments. The selective embolization procedure preserves the segments of the liver to remain and promote its compensatory hypertrophy. In the present case, the procedure consist of embolizing the right segments of the liver.
The procedure includes two main steps: a biliary drainage to prepare the patient for surgery and the embolization itself. Access to the portal vein is performed through a lateral percutaneous puncture under ultrasound guidance.
A portography, or image of the injection of contrast agent into the portal circulatory system, is performed. This injected fluoroscopic image allows for mapping the liver and identifying the vessels in the anatomical region of interest. It enables ultra-selective micro-catheterization of the liver vessels. The navigation of the endovascular tools in the liver is done in roadmap mode based on the previously performed angiography. This method allows selective and specific access to the different small branches of the portal system. An ultra-specific embolization of all the vessels and micro-vessels in the right part of the liver is then performed using biological glue. This glue helps to obstruct particularly fine vessels. Once all the vessels are obstructed, a final angiographic control is performed to ensure that the vessels are properly obturated and that blood flow no longer irrigates the part of the liver that will be removed.
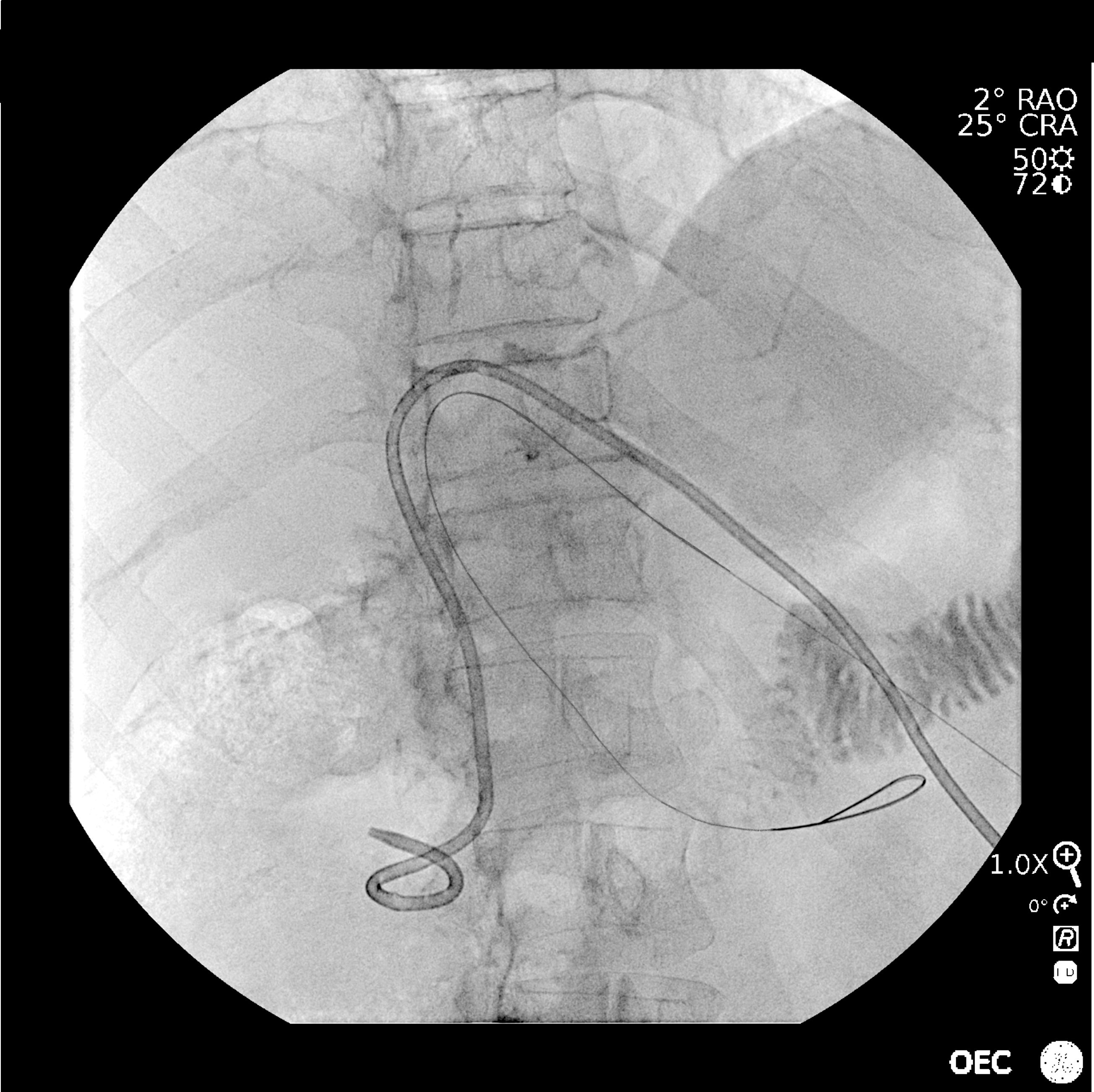
Step 1: Biliary Drainage
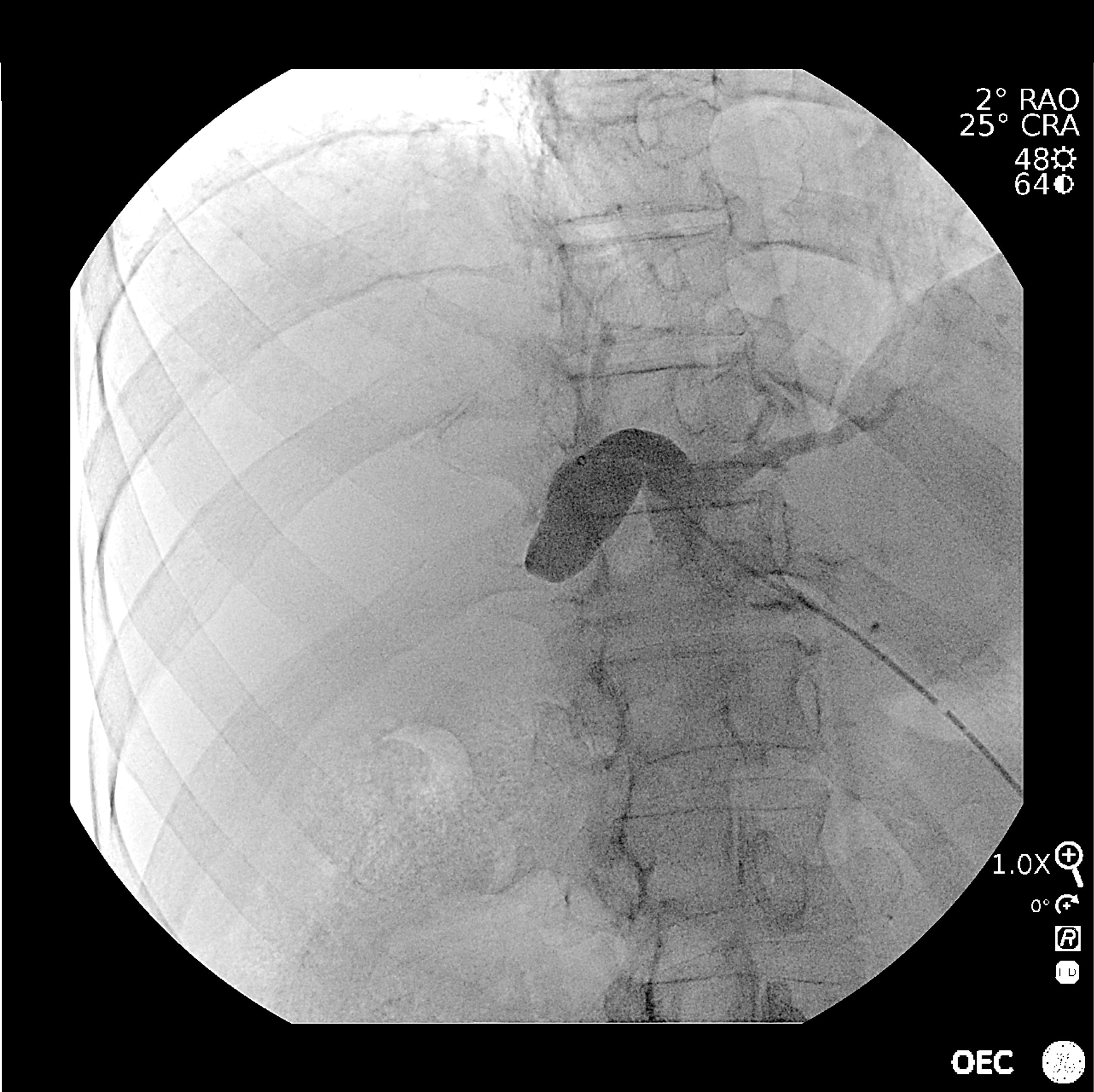
1. Biliography confirming the puncture of the biliary tract (by percutaneous access).
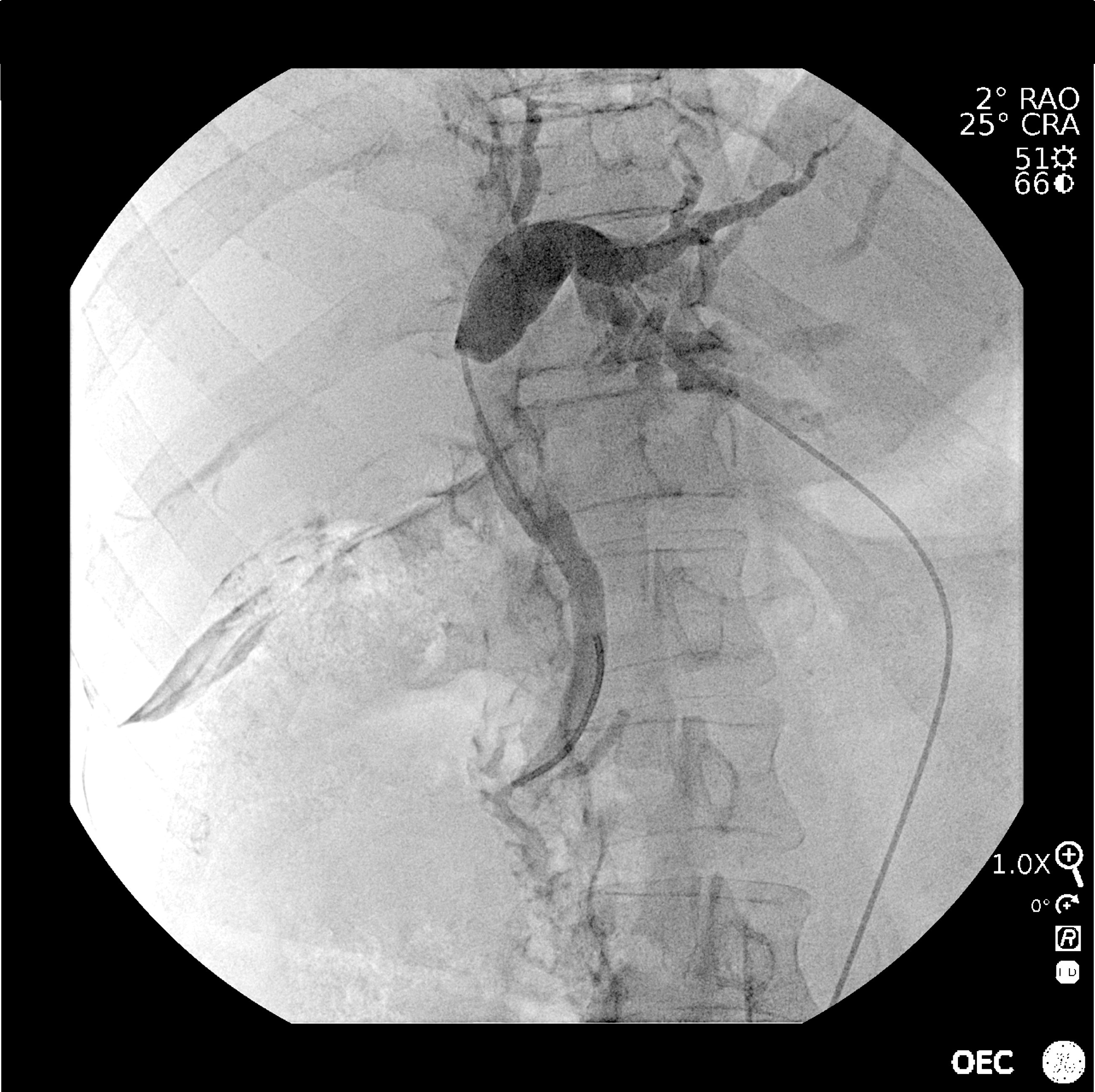
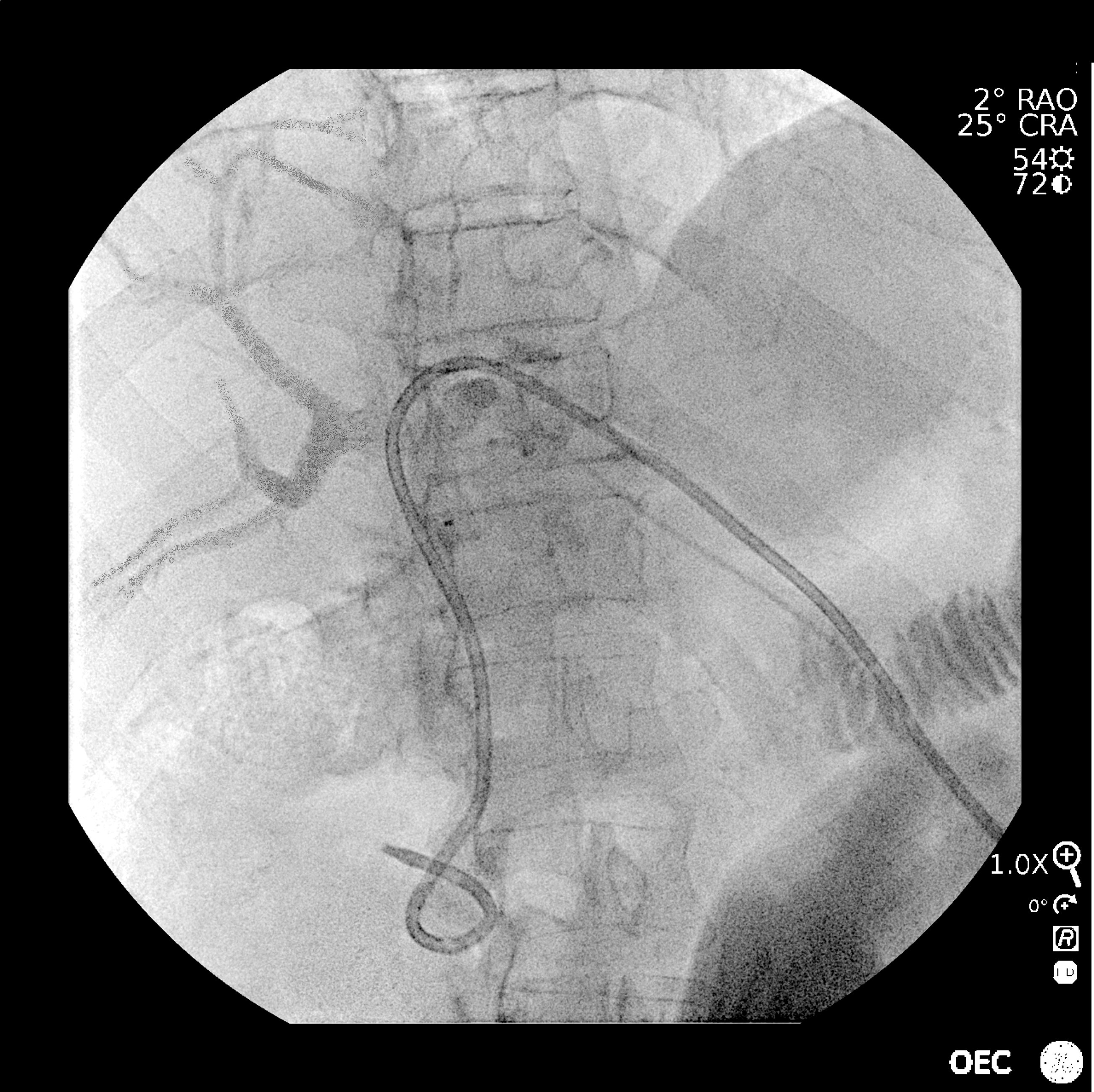
2. Biliography of the navigation of the guidewire to the duodenal papilla.

3. Biliography for the navigation of the guidewire to the duodenum.

4. Biliography confirming the placement of the drain inside the duodenum.
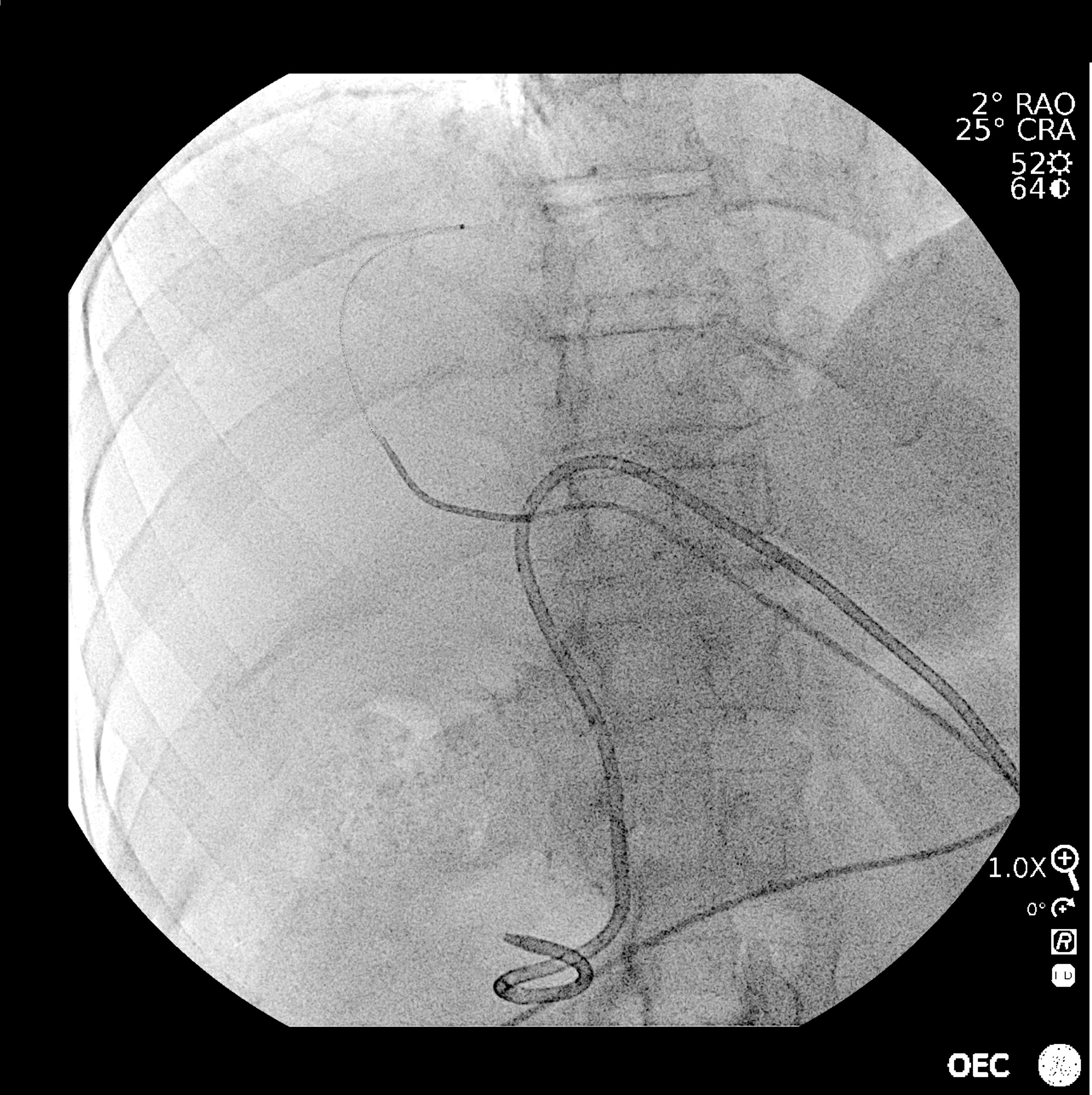
Step 2: Embolization of the portal system
5. Fluoroscopy during portal system puncture.
6. Angiography confirming the position of the catheter in liver.

7. Digital Subtracted Angiography of the portal system.
8. Angiography at the beginning of the ultra-selective embolization of the portal system.
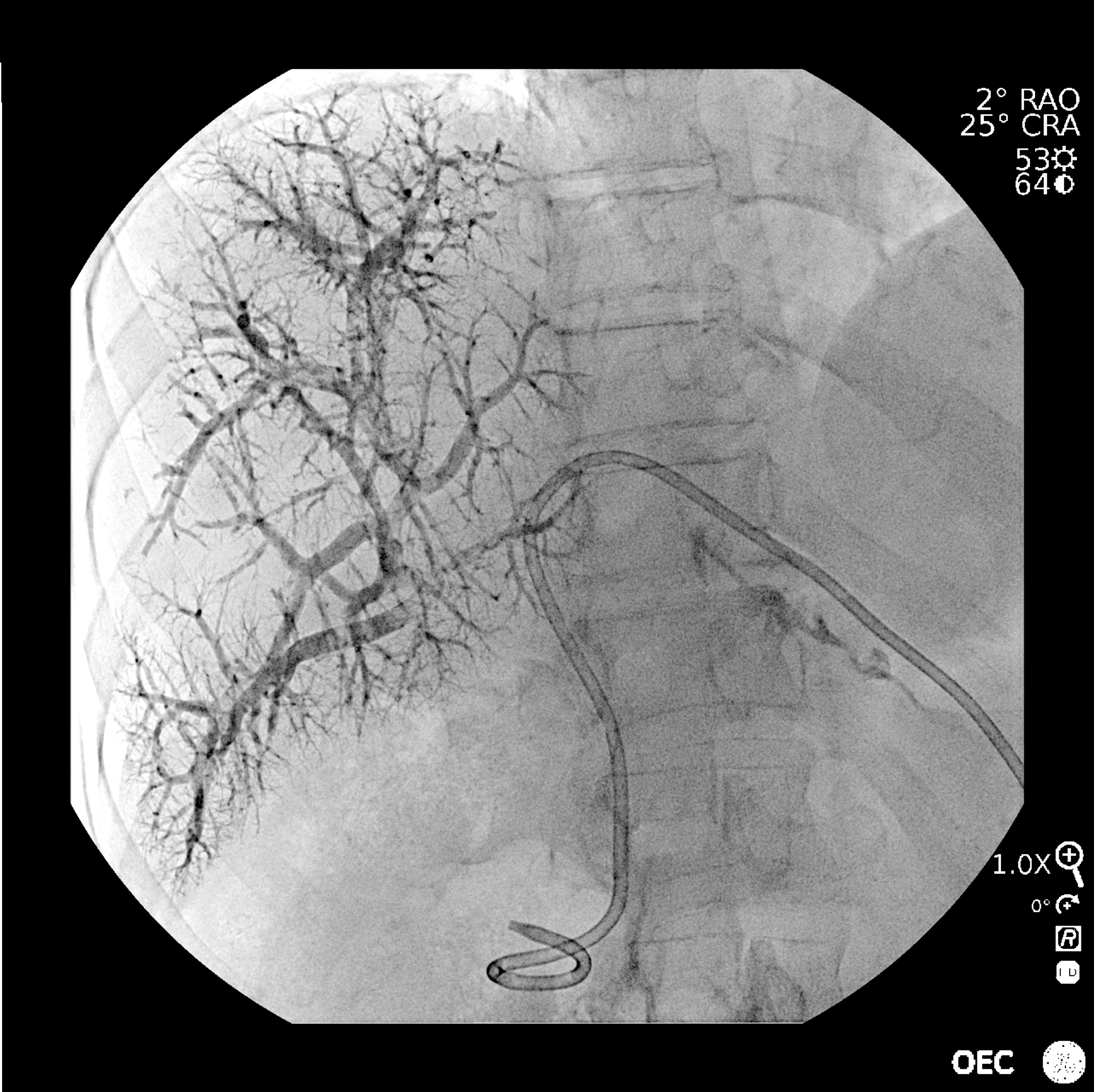
9. Portography of final control showing obstruction of the portal system of the right part of the liver to be resected.
Dr. Ben Cheikh is a paid consultant for GE HealthCare and was compensated for participation in this testimonial. The statements described here are based on Dr. Ben Cheikh own opinions and on results that were achieved in his unique setting. Since there is no “typical” hospital and many variables exist, i.e. hospital size, case mix, etc.. there can be no guarantee that other customers will achieve the same results. JB08399XE